Reduce Risk, Standardize the Procedure and Create an Elliptical Ventricle … Every Time.
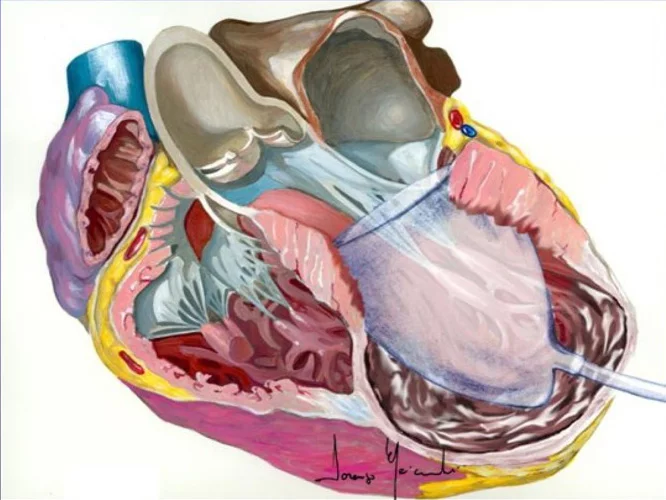
“A ventricle sizing device is one of the most important parts of the operation to ensure a properly sized and shaped ventricle.”
The Surgical Ventricular Restoration (SVR)® procedure is a comprehensive surgical technique utilizing the Mannequin device to treat patients suffering from ischemic heart failure. This comprehensive surgical procedure enables surgeons to create an elliptical ventricle, with repeatable and optimal outcomes every time. Patient after patient. Chase Medical is passionate about Surgical Ventricular Restoration, because we have seen first-hand the benefits of SVR for heart failure patients around the globe.
Chase Medical works closely with distinguished physicians such as: Lorenzo Menicanti, M.D., and others who continue to advance the surgical technique for SVR. Chase Medical sponsors educational programs in the U.S. and in Europe to promote SVR surgical best practices.
Our goal is to encourage the use of a standardized procedure for surgical consistency while reducing risk and variability.
The ideal procedure for any surgeon is one that is time-tested, repeatable and generates optimal outcomes for their patients. The proper surgical technique using the Mannequin creates an elliptical ventricle every time – patient after patient.
The SVR procedure is being performed around the world.
Longitudinal profile of NT-proBNP levels in ischemic heart failure patients undergoing surgical ventricular reconstruction: The Biomarker Plus study
Serial profiles (either in increasing or in decreasing) at different time points are associated with a modulation of the risk of adverse events and, therefore, are important indicators for monitoring the evolution of the disease, even after cardiac surgery.
Myocardial reconstruction in ischaemic cardiomyopathy
An increase in left ventricular volume after a myocardial infarction is a key component of the adverse remodelling process leading to chamber dysfunction, heart failure and an unfavourable outcome.
Restrictive filling pattern in ischemic cardiomyopathy: Insights after surgical ventricular restoration
RFP was reversed after SVR in 22 of our 43 patients with ICM with a response that remained stable over time, associated with improved New York Heart Association class.
Surgical Ventricular Restoration for Ischemic Heart Failure: A Glance at a Real-World Population
Surgical ventricular restoration (SVR) has repeatedly been suggested as a viable therapeutic strategy for ischemic heart failure (HF) patients, although the survival benefit is still debated. We investigated a real-world population treated with SVR in a single center with high case volumes.
Comparable outcomes between genders in patients undergoing surgical ventricular reconstruction for ischaemic heart failure
In this study, long‐term outcomes for women and men with ischaemic HF undergoing complex cardiac surgery were equivalent. Albeit older and more symptomatic, women should not be denied this type of cardiac surgery.
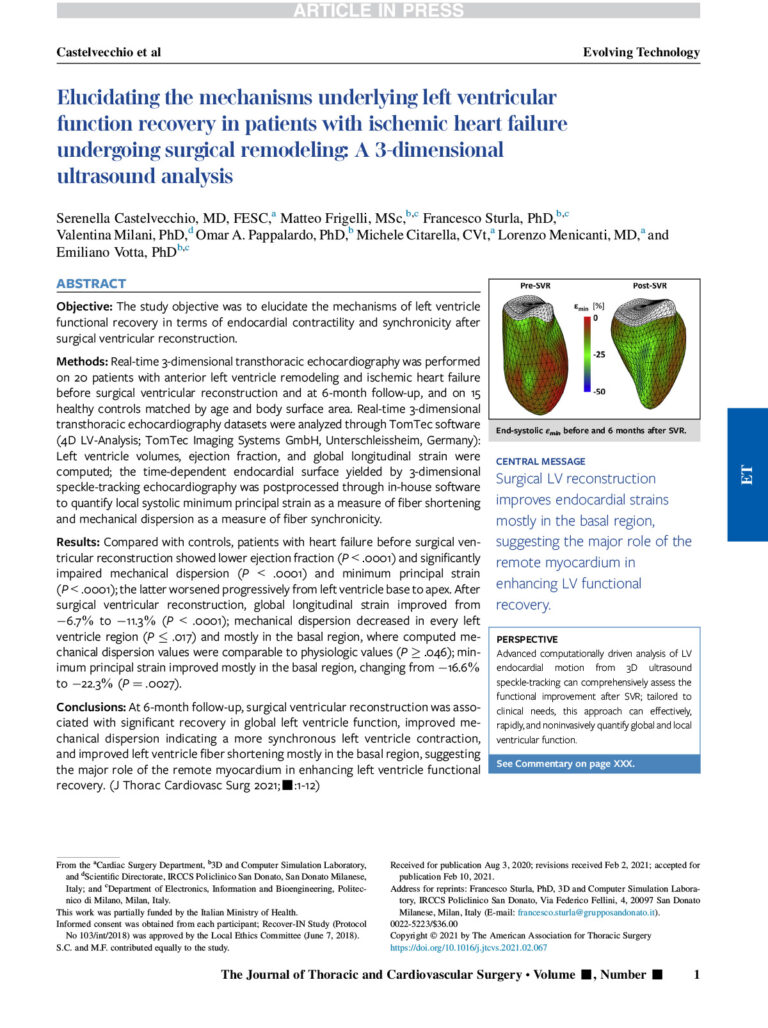
Elucidating the mechanisms underlying left ventricular function recovery in patients with ischemic heart failure undergoing surgical remodeling: A 3-dimensional ultrasound analysis
Surgical LV reconstruction improves endocardial strains mostly in the basal region, suggesting the major role of the remote myocardium in
enhancing LV functional recovery.
A critical outcome of any procedure to treat heart failure must be to reduce ventricular wall stress, stop the disease progression, and restore contractile function to the heart.
The Law of Laplace is a generally held law of physics that clearly describes the factors that determine wall stress increases or decreases in a vessel (the ventricle):
The Law of Laplace Wall Stress = (Pressure in Ventricle) x (Ventricle Radius) 2 (Wall Thickness)
In the HF patient, all of the variables (pressure, ventricle radius and wall thickness) conspire to increase wall stress. The left ventricular pressure rises as more volume enters the ventricle. The radius increases as the ventricle dilates into a sphere to accommodate the increasing volume. The wall thins as the ventricle dilates.
Restoring the size of the ventricle to near its “normal” size (reducing its volume) is one factor in reducing the wall stress.
More importantly, restoring the ventricle to an elliptical chamber is a critical factor to reduce wall stress by decreasing the radius of the dilated ventricle.
Correctly orienting all of the constituent components of the ventricle, i.e. aortic valve, mitral valve apparatus and papillary muscles, helps ensure optimal performance.
SVR System Reimbursement Reference
Medicare assigned a code specifically for the Surgical Ventricular Restoration (SVR) procedure. CPT Code 33548 describes the SVR procedure utilizing a patch and a shaping device, such as the Mannequin.
CPT Code
CPT 33548
Restore/remodel, ventricle
MS-DRG Codes (formerly DRG 108)
MS DRG Code 228
Other cardiothoracic prodecures with MCC (major complications or co-morbidities)
MS DRG Code 229
Other cardiothoracic prodecures with CC (complications or co-morbidities)